The Lapiplasty procedure is a modern approach designed to correct bunions at their source, restoring natural foot alignment in three dimensions.

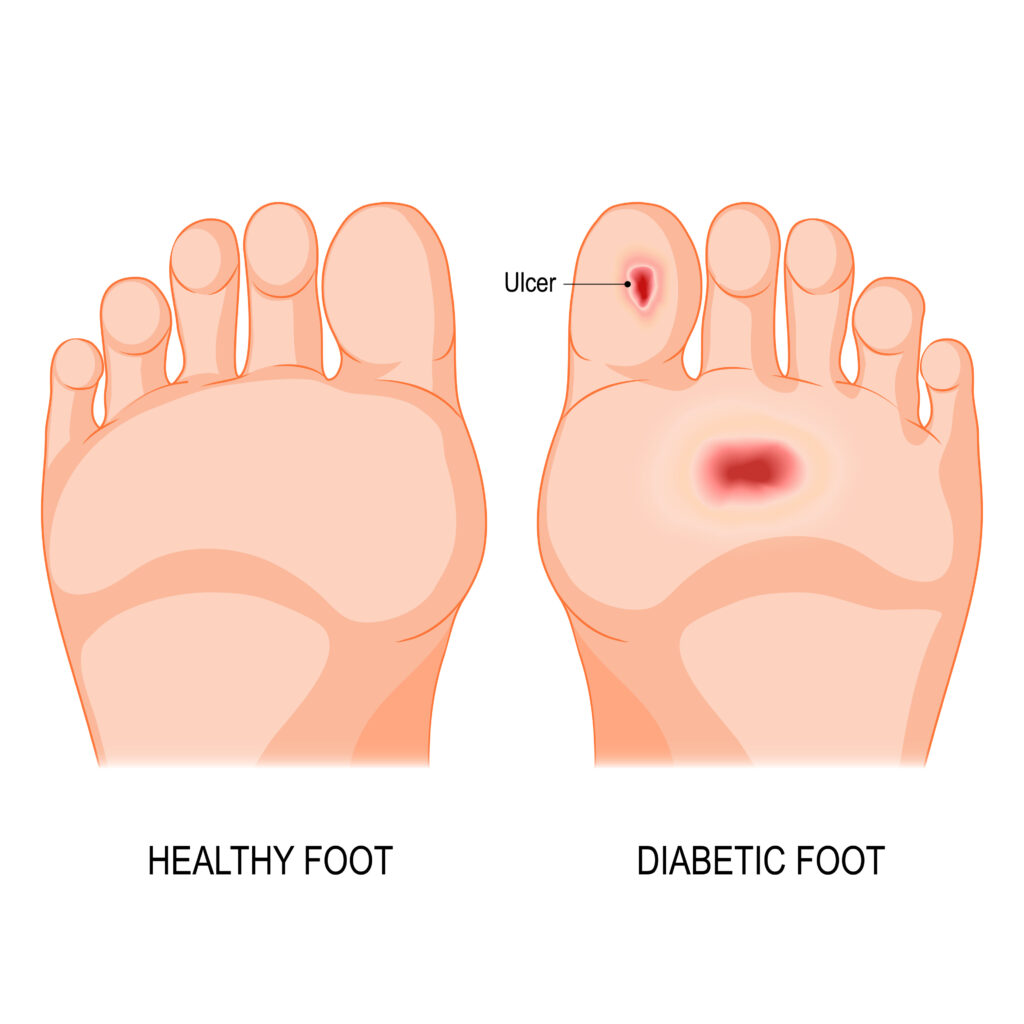
Diabetes can cause nerve damage (neuropathy) and reduced blood flow, making small cuts turn into serious wounds that are slow to heal. Our orthopedic foot and ankle specialists help protect joints, correct deformities, and restore function while coordinating vascular, wound-care, and endocrine support for true limb preservation.


Reducing mechanical stress is central to healing diabetic foot ulcers. Non-removable devices—like total contact casts (TCCs)—have the strongest evidence for faster healing compared with removable boots or specialty shoes. We select the safest, most effective offloading method for your lifestyle and ulcer location.



When an ulcer keeps coming back because bone or alignment is the problem, we start with the smallest fix that truly removes pressure. Often a quick, low-incision procedure does the trick; if not, we step up to sturdier reconstruction to protect you long-term.
Common Minimally invasive treatment options
If minimally invasive isn’t the best fit
Daily habits dramatically cut your risk:
Can diabetic foot ulcers really heal?
Yes—especially when pressure is truly offloaded, wound care is consistent, circulation is adequate, and infection is controlled. Non-removable offloading like TCCs has the strongest evidence for higher healing rates and shorter time to closure.
Do I always need antibiotics for a foot ulcer?
No. Uninfected ulcers don’t typically need antibiotics. When infection is suspected, guidelines recommend deep tissue cultures after debridement and targeted therapy based on severity and organisms.
What if I have Charcot foot?
Early recognition and immobilization/offloading are crucial. Once inflammation quiets, surgical reconstruction may be considered to restore a plantigrade, braceable foot and prevent recurrent ulcers.